The Truth About Lip Flip
There's a treatment that keeps circulating on social media as a "quick, affordable alternative" to lip filler: the lip flip. A few units of neuromodulator into the upper lip, and the lip is said to appear fuller by rolling slightly outward. It sounds simple. It sounds low-commitment. Neither of those things make it a good idea.
Sharief Aesthetics doesn't offer this treatment. Here's the clinical reasoning, plainly stated.
What a Lip Flip Actually Does
A lip flip works by weakening the orbicularis oris, the ring-shaped muscle that circles the mouth. This isn't a decorative muscle. It's the muscle responsible for three things you use dozens of times a day without thinking about them: sealing your lips completely, pursing them into a round shape, and articulating certain speech sounds with precision.
A lip flip doesn't add volume. It doesn't fill anything. It works by partially disabling the very muscle that gives your lips their function, so that the upper lip relaxes into a slightly more rolled, fuller-looking position at rest.
The visible change is real. So is the trade-off.
In my opinion, lip flip is fake lips. Not a treatment, an illusion, and the patient is the one who pays for it.
What Gets Traded Away
For four to six weeks, the duration of the neuromodulator's effect, the upper lip doesn't work the way it used to.
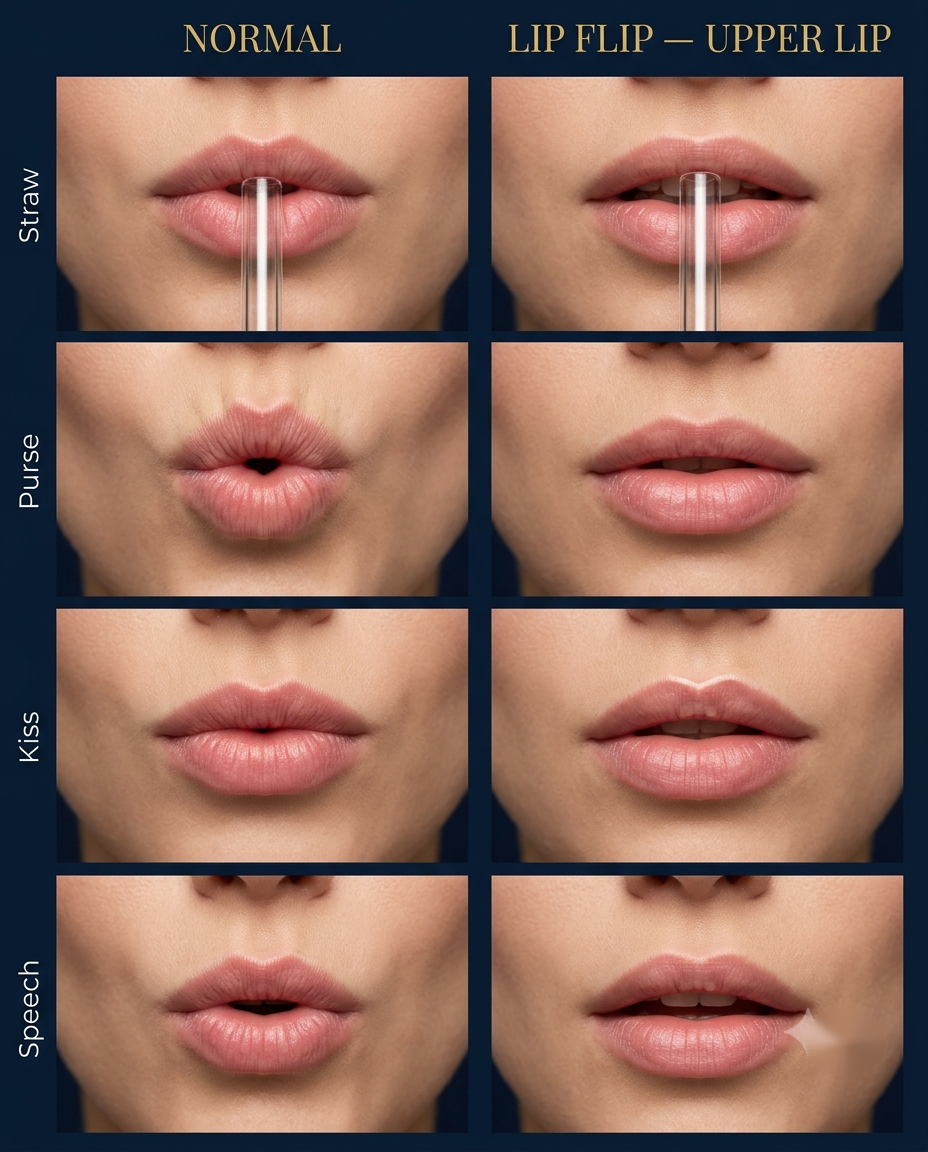
- Drinking through a straw requires a complete seal around it. A weakened upper lip can't always close that gap.
- Pursing the lips, for a whistle, for blowing out a candle, for certain instrument playing, requires the same full-circle muscle contraction that's now been chemically reduced.
- Speech sounds that rely on a firm lip seal, the consonants that need the lips to close completely before releasing, can come out softened or imprecise.
None of this is dramatic or disfiguring. It's subtle. Which is, in a way, the problem: patients often don't fully appreciate how much they rely on precise lip function until it's temporarily reduced, and by then there's no way to reverse it early. Neuromodulator effects wear off on their own schedule, not on request.
Why We Don't Offer It
At Sharief Aesthetics, we don't offer lip flip. Two reasons, both clinical:
It's a function trade-off, not an enhancement. The change comes from disabling movement, not from restoring volume or structure. We think a treatment that temporarily limits a patient's ability to eat, speak, and drink normally needs a stronger justification than a subtle cosmetic shift, and for us, it doesn't clear that bar.
The injection sites carry a real margin-of-error problem. The points typically used near the corners of the mouth sit close to muscles responsible for smile symmetry. Diffusion beyond the intended target in this area can affect those muscles too, and the result can look like an uneven or asymmetric smile, a separate, unwanted complication layered on top of the lip's reduced function. The anatomical margin here is tighter than we're comfortable working within for the aesthetic gain on offer.
This is a clinical judgment specific to our practice, not a comment on any other provider's skill or technique.
What We Recommend Instead
If the goal is fuller, more defined lips, our approach is dermal filler, specifically our VVL (Vertical Vector Lip) technique, which builds structure and volume vertically rather than simply widening the lip horizontally. It adds what's actually missing instead of disabling what's already there, and it doesn't come with a four-to-six-week window of reduced lip function.
Every patient's anatomy and goals are different, which is exactly why this starts with a real consultation, not a menu item.