The Truth About Melasma Treatment
Melasma is one of the most common pigment concerns people bring to a clinic — and one of the most commonly mishandled. It appears as patches of brown or grey-brown, usually across the cheeks, forehead, upper lip or jawline, often in a near-symmetric pattern on both sides of the face. People try cream after cream, sometimes treatment after treatment, and watch it fade a little, then return — or come back darker.
The frustration is real. And most of it traces back to a single, fixable problem: melasma is misunderstood, frequently at the very first step — the diagnosis.
It isn’t a stain. It’s a patch of skin behaving differently.
The most useful thing to understand about melasma is also the thing most often missed. It is not a mark sitting on the surface that you can scrub, bleach or burn away. It is a chronic pigment disorder — a patch of skin where the pigment-making machinery has been switched into overdrive and stays there.
And it isn’t one rogue cell doing it. When you read the underlying science, melasma looks far less like a stain and far more like a small neighbourhood of skin where everyone is signalling everyone else to make more pigment: the pigment cells themselves, the surrounding skin cells that talk to them, the deeper support cells, even the tiny blood vessels feeding the area. They keep one another switched on. That is precisely why a single product aimed at the pigment alone so rarely settles the whole thing. You are not treating a spot — you are calming a process that several parts of the skin are driving at once.
That process has three usual ingredients working together: a genetic tendency, hormonal influences such as pregnancy, the oral contraceptive pill or hormone therapy, and exposure to light and heat. That combination is why melasma behaves the way it does — symmetric, patterned and persistent — and why no single cream tends to be the whole answer.
The most common reason treatment “fails”: the diagnosis
Here is the part most people — and not only patients — get wrong. Two very different conditions are routinely confused: melasma and post-inflammatory hyperpigmentation, or PIH.
PIH is pigment left behind after the skin has been inflamed or injured — by acne, a rash, a scratch, or a procedure. It has a clear cause, and it follows the map of that cause. Melasma, by contrast, arises on its own, driven by the factors above. The two can look alike, often occur together, and respond to completely different plans. Treat one as if it were the other and you are working against the problem from the first day.
Why depth changes everything
There is a second layer to the diagnosis, and it is the one that explains most of melasma’s reputation for being stubborn: how deep the pigment sits.
Think of a stain on a sheet of paper. If it sits on the surface, you have a fair chance of lifting it. If it has soaked through into the layer beneath, no amount of rubbing the top will reach it. Skin works in much the same way. There is a thin boundary between the upper and lower layers of skin, and in melasma that boundary is often broken down — which lets pigment drift deeper than it should. Pigment that stays high responds reasonably well. Pigment that has dropped deeper is far more stubborn, and it is also far more common in richer skin tones.
This single fact quietly explains nearly everything frustrating about melasma: why it shrugs off creams, why it keeps coming back, and why an aggressive procedure can spend its energy on pigment it was never going to reach. Which is why establishing what the pigment is, and how deep it sits, before anything else, is not a formality. It is the treatment.
Why skin tone changes the plan
For deeper skin tones — Fitzpatrick types IV, V and VI — the stakes are higher in both directions. Richer melanin carries a greater tendency toward pigment problems in the first place, and the pigment cells react more strongly when provoked.
That second point is the one that catches people out. Treatments that comfortably lift a sun spot from fair skin — strong lasers, intense light, deep peels — can do the opposite on darker skin, triggering more pigment rather than less. Skin tone is a genuine limiting factor on which treatments are appropriate, and a responsible plan is built around it, not in spite of it.
The trap: why treating it hard backfires
The instinct, faced with stubborn brown patches, is to hit them hard. With melasma, that instinct is the trap.
Melasma skin is already irritable — primed to react. Heat, intense light and harsh peels can tip it over the edge, and inflamed melasma skin answers the only way it knows how: by making more pigment. You can end up with fresh pigment laid down on top of the melasma you set out to lighten, and a result that is worse than where you started. This is why heat- and light-based treatments, including IPL, are approached with real caution in melasma and are not a first move. It is also why ordinary heat — not only the sun — can stir it up. There is no setting strong enough to overpower the underlying process; pushed too hard, it pushes back.
The honest part: managed, not cured
This is the truth the title promises. There is no permanent cure for melasma. It is a chronic, relapsing condition. With the right, patient approach it can be meaningfully lightened and kept under control — but it tends to return, particularly with sun, heat and hormonal triggers. Anyone promising to erase it permanently in a session or two is not being straight with you.
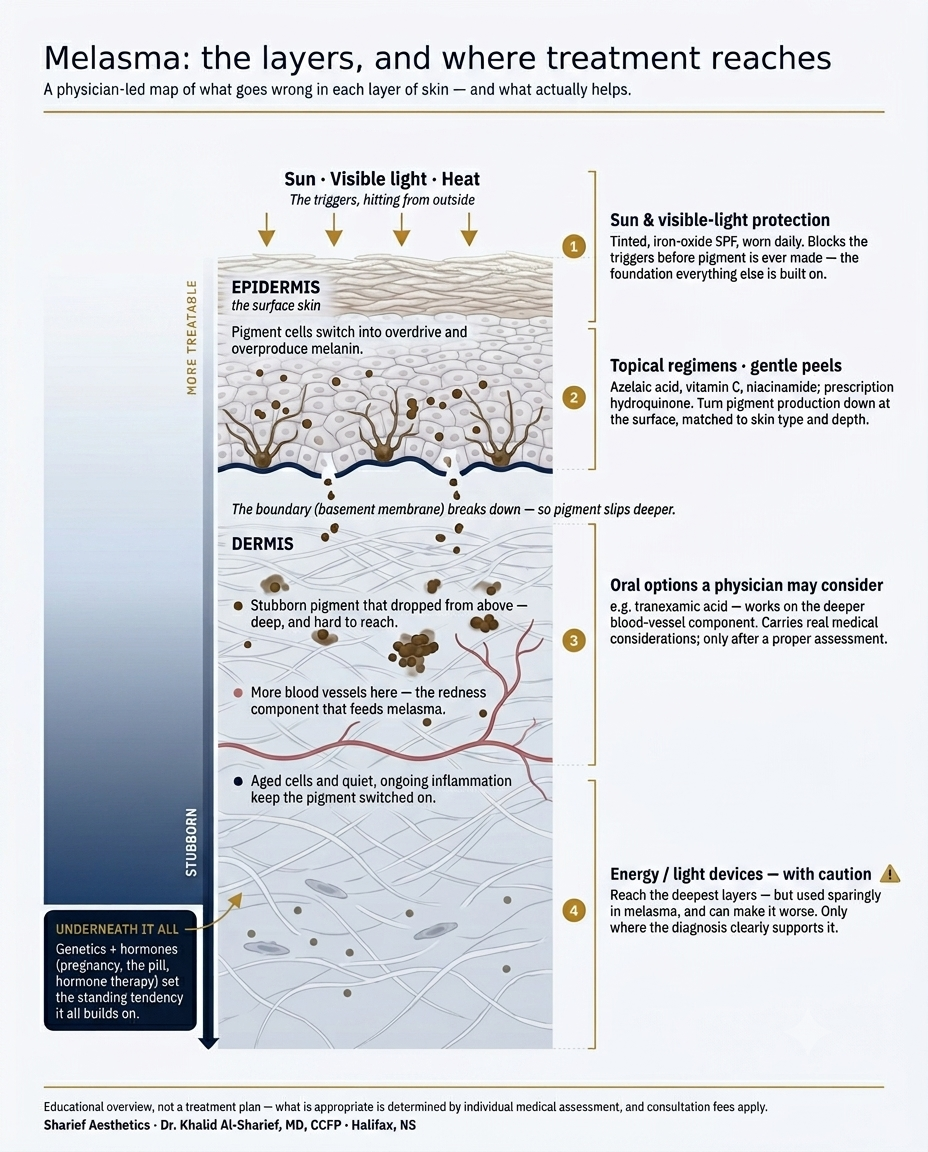
The realistic goal is control and maintenance — and the single most important, most underused part of that is protection. Not protection from UV alone. Melasma is driven by visible light and heat as well, which ordinary sunscreens don’t fully address. Broad-spectrum cover that also blocks visible light — the tinted, iron-oxide formulations — worn daily and year-round, is the foundation everything else is built on. Without it, every other treatment is working against the tide.
So what actually helps?
Once the diagnosis is clear, melasma is managed in layers — gentlest and most foundational first. There is no single hero treatment; the steady results come from combining a few quiet measures and staying consistent. In rough order:
Protection comes first. Daily broad-spectrum cover that also screens visible light — the tinted, iron-oxide sunscreens described above — is the base every other measure is built on. Skip it, and everything else is working against the tide.
Topical regimens that turn the pigment machinery down. A number of well-studied ingredients work by gently slowing the steps the skin uses to make pigment — examples include azelaic acid, vitamin C and niacinamide, and, in prescription form and under medical supervision, agents such as hydroquinone. The point is never the single product; it is the right combination, matched to your skin type and the depth of the pigment, used patiently and adjusted over time. These are usually the workhorses of melasma care.
Carefully chosen in-clinic options — where the diagnosis supports them. Gentle, superficial treatments such as mild chemical peels can have a role for the right person. Stronger energy- and light-based devices are used sparingly and selectively in melasma, for the reasons explained above, and only when the assessment genuinely calls for them. With melasma, restraint is not caution for its own sake — it is the strategy.
Time and maintenance. Melasma rewards patience and punishes shortcuts. Improvement is gradual, and keeping it lightened is an ongoing job rather than a one-off. The plans that hold are the ones built to be sustained.
One thing worth saying plainly: some of the options that help melasma — including oral medications such as tranexamic acid that a physician may consider — carry real medical considerations and are only appropriate after a proper assessment. That is one more reason melasma is better handled as a medical condition than a cosmetic errand.
“I treat superficial, sun-related pigment with care. But where deeper skin tones and true melasma meet — Fitzpatrick IV–VI — I refer to dermatology first. Knowing when to bring in a specialist is part of the same standard that protects your skin”
— Dr. Khalid Al-Sharief, MD, CCFP
How we approach melasma at Sharief Aesthetics
At Sharief Aesthetics, melasma is treated as the medical condition it is. As a physician-led clinic, the assessment begins by establishing what the pigment actually is — melasma, PIH, or both — and how deeply it sits, because that determines everything that follows.
From there the approach is deliberately conservative: gentle and layered, topical-led where appropriate, with energy-based treatments used carefully and only where the diagnosis genuinely supports them. The aim is steady, lasting control while protecting your skin — and an honest conversation, from the very start, about what melasma will and won’t do.