The Truth About an Uneven Smile After Botox-Type Injections
There is a treatment I was trained to perform, that I know how to perform well, and that I do not offer: DAO correction — treating the Depressor Anguli Oris to soften a downturned mouth. Not because I can't. Because of what I've seen happen when it goes wrong — and because I don't think the wrong is being counted correctly in the first place.
It's standard technique in every aesthetics course, taught with a stated complication rate that sounds low enough to be an acceptable risk for a modest cosmetic gain. I want to explain why I think that number is measuring the wrong thing — and why some patients end up with an uneven smile after a neurotoxin injection with no clear explanation for why.
What DAO Is Supposed to Fix
The Depressor Anguli Oris is the muscle that pulls the corners of the mouth down. Overactive, it contributes to a permanently downturned, tired, or unhappy resting expression — the look some patients describe as “resting sad face.” Relaxing it with a neurotoxin injection is meant to let the corners of the mouth sit slightly higher at rest.
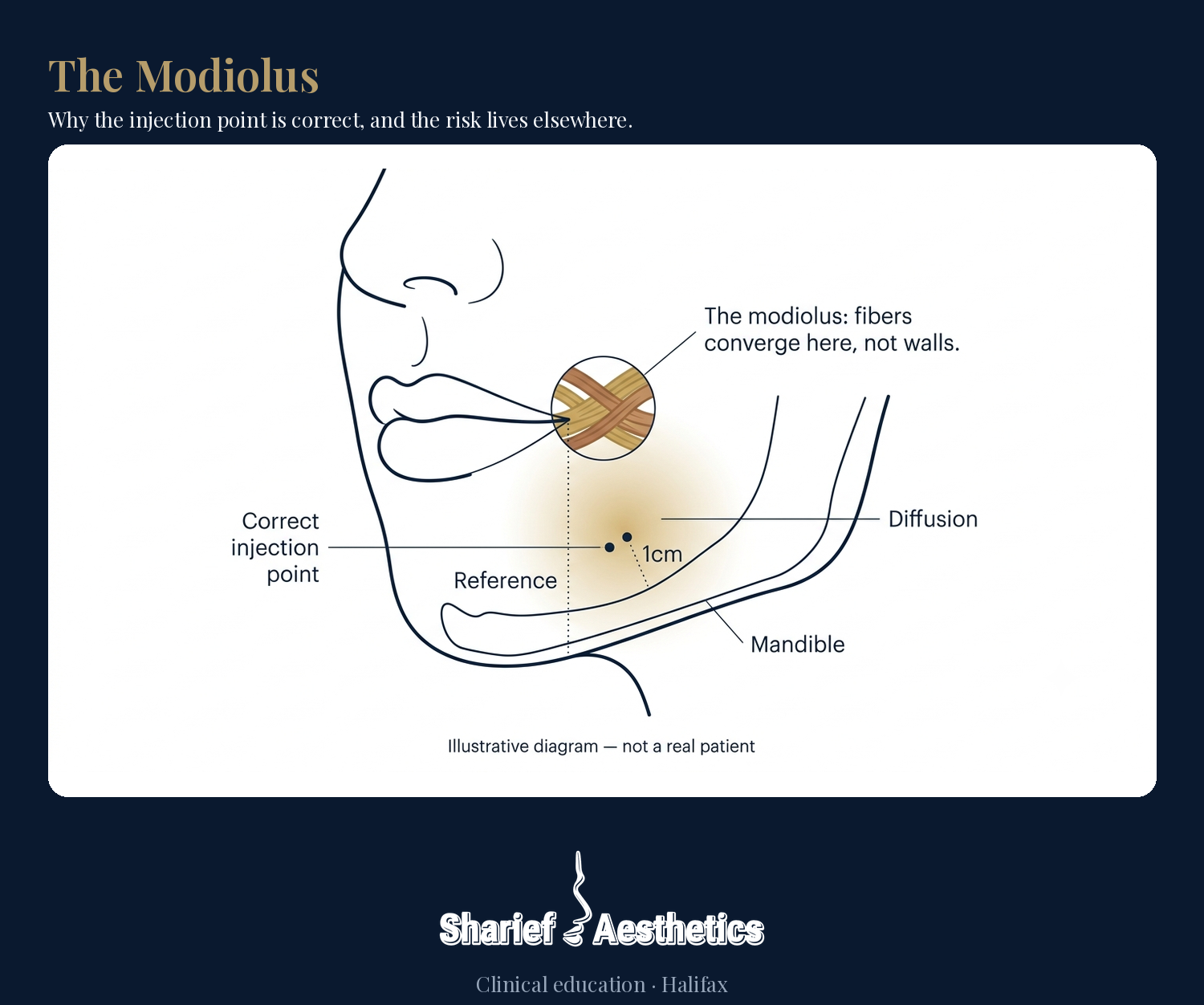
Standard technique is precise about where to inject: draw a line from the corner of the mouth down to the jawline, then place the injection lateral to that line, roughly 1cm above the bone. Done exactly this way, the needle sits correctly in the DAO. That part isn't in question, and it isn't where the risk actually lives.
Why Correct Technique Still Isn't Enough
Standard teaching correctly identifies where to inject and where not to — draw the line, find the dimple, stay lateral, avoid the X. What it doesn't typically explain is why staying inside that safe zone isn't a guarantee. Here's the part that doesn't get explained clearly enough. Near the corner of the mouth, several muscles — DAO, the Depressor Labii Inferioris (DLI, which controls the lower lip during speech), orbicularis oris, risorius, and buccinator — converge at a single point called the modiolus. At that point, the muscles don't sit in separate, walled-off compartments. Their fibers physically interweave.
That matters because neurotoxin doesn't stay exactly where the needle tip was. It diffuses outward through the tissue it's placed in. An injection placed correctly in the DAO belly, 1cm off the bone, lateral to the landmark line, can still reach fibers that functionally belong to the DLI — not because the needle drifted, but because there's no clean wall between the two muscles at the one point where precision matters most.
This is also why the specific product matters, though the mechanism applies across every neurotoxin brand on the market. Diffusion is the defining strength of some formulations over others — it's what makes them forgiving and easy to blend everywhere else in the face. At the modiolus, that same spread works against you: the more a product diffuses, the more likely correctly placed toxin still reaches the neighboring muscle anyway.
The Complication Nobody's Counting Properly
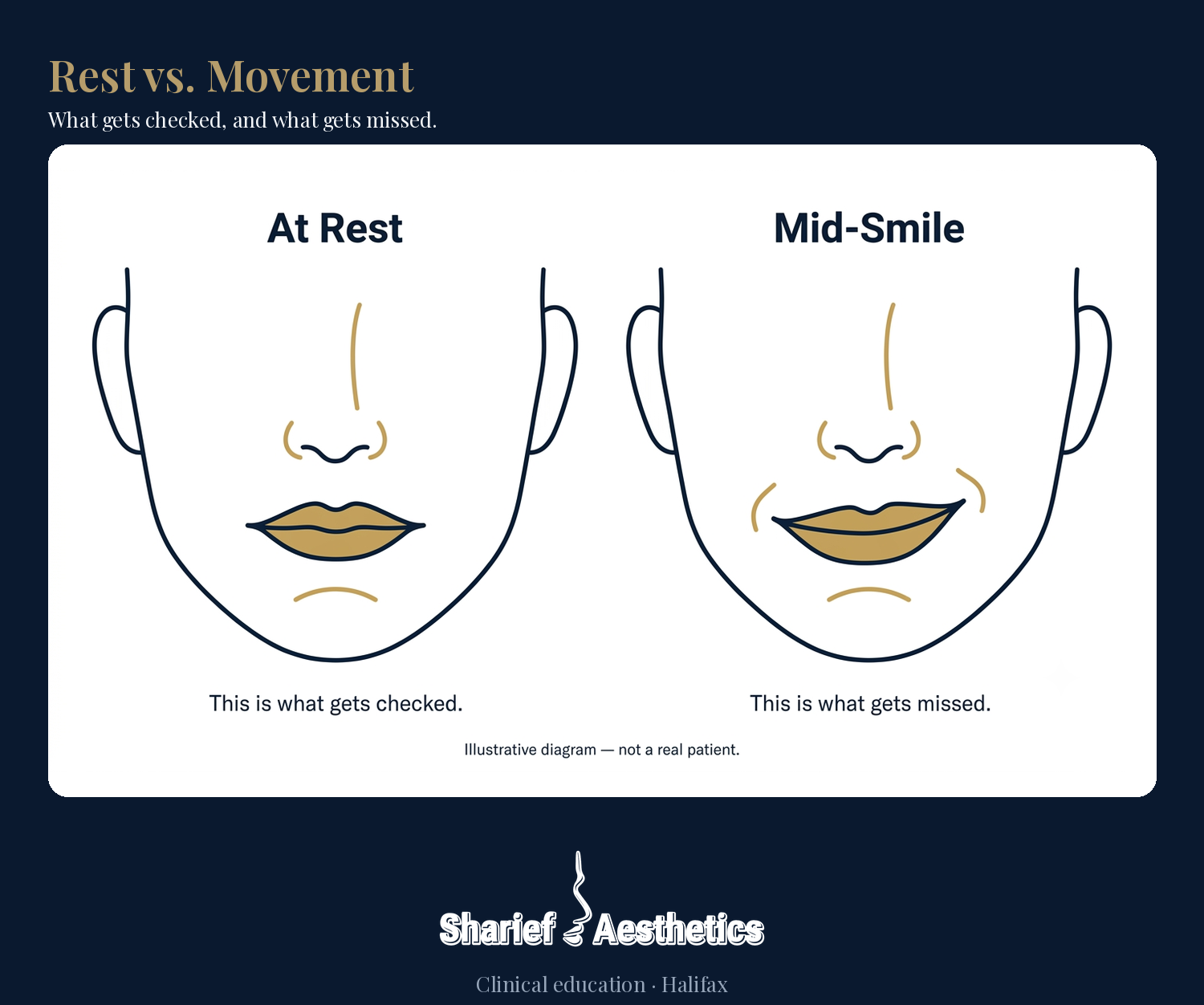
When toxin reaches the DLI, the result is rarely a droop you'd notice with the face at rest. It's a dynamic asymmetry: one side of the lower lip doesn't move quite the same as the other when the patient talks, laughs, or smiles.
That distinction matters more than it sounds like it should. A static droop is obvious in the mirror. Patients notice it, report it, and it gets logged as a complication. A dynamic asymmetry that only shows up mid-sentence or mid-laugh is a completely different thing to catch. Many patients don't clock it as a complication at all — they just notice their smile looks slightly different lately, and move on, or assume it's unrelated to a treatment they had weeks ago.

If the standard method of tracking this complication mostly catches the static cases and misses the dynamic ones, then the published rate isn't wrong exactly — it's incomplete. It's counting the version of this problem that's easy to see, not the version that's actually more common.
Why I Don't Offer It
In my own clinical experience — including cases referred to me after the fact — this dynamic asymmetry shows up far more often than the commonly cited numbers suggest. To be precise: that's my own clinical observation, not a published incidence figure. No published number measures the dynamic presentation separately from the static one — which is exactly the gap I'm describing.
Given that, the math doesn't work for me. The aesthetic gain from softening a downturned mouth is real but modest. The risk of a mouth that moves unevenly every time a patient speaks or smiles — for weeks, until the treatment wears off — is not a trade I'm willing to make on a patient's behalf, especially when the anatomy itself, not an error in anyone's hands, is what makes the risk hard to avoid.
This isn't a comment on any injector's skill or technique, and it isn't specific to any one brand of neurotoxin. The landmarks are correct, the injection point is correct, and the risk is still there — because at the modiolus, correct technique and an adverse result aren't mutually exclusive. That's exactly the point this article is making.
What This Means for You
If you're looking into DAO correction, or if you've noticed an uneven smile after a neurotoxin treatment elsewhere, ask directly: how is the complication rate you're being quoted actually measured? Is it tracking how the mouth looks at rest, or how it moves when you talk? If the answer is “at rest,” you're not getting the full picture — and neither, in most cases, is the person quoting it to you.
None of this is meant to talk anyone out of a treatment they want. Our job isn't to scare you away from something — it's to make sure you're deciding with the full picture, not a partial one. Once you know the risk, the choice is yours to make.
And if you're one of the people currently living with this, here's what matters most:
It passes. It's not permanent. It happens. Now you know, and you can decide.
On the timeline: it resolves the same way the treatment itself wears off elsewhere in the face — and it may take a little longer than that to fully settle. There's no published number specific to this particular presentation; general neurotoxin duration is the closest honest reference point available.
At Sharief Aesthetics, we'd rather tell you why we've made a call than simply say no and leave it there. This is one of those calls.