The Truth About Vasculaze: A Physician's Guide to Vascular Lesions
In thirty years of medicine — most of it in emergency departments where vascular emergencies were a daily reality — I developed a deep respect for the complexity of the vascular system. When I transitioned into aesthetic medicine, I brought that same clinical precision with me.
What I found in the aesthetic space surprised me.
The word "vascular lesion" is used as a single catch-all category for conditions that are biologically, anatomically, and clinically quite different from one another. A spider vein on the cheek and a deep hemangioma on the trunk are both called "vascular lesions." They are not the same thing. They do not respond the same way. They do not carry the same risk profile. And they should not be approached with the same protocol.
This matters because the device used to treat them — Vasculaze — is a powerful clinical tool that delivers targeted laser energy to hemoglobin within blood vessels. When used with proper patient selection and clinical judgment, the results are excellent. When used indiscriminately, the outcome can be poor at best and harmful at worst.
This article is a physician's honest guide to what Vasculaze can treat, what it cannot, and why the distinction matters to you as a patient.
The Classification Problem
The medical community has been classifying vascular anomalies since 1982, when Mulliken and Glowacki published what became the foundational classification system still used today. Their insight was simple but profound: vascular anomalies are either tumours (which grow and may involute) or malformations (which are structural errors present from birth and never resolve on their own).
This distinction is not academic. It determines everything — the natural history of the lesion, the appropriate treatment, and the expected outcome.
Most aesthetic clinics and, frankly, most device marketing materials do not make this distinction. They show a red spot before and a clear complexion after, and call it a day. As a physician, I am not able to approach patient care that way.
What follows is a practical guide to the six vascular lesion types you are most likely to encounter, and what a physician-led approach looks like for each.
1. Telangiectasia and Spider Veins
Telangiectasias are dilated superficial capillaries — tiny blood vessels that have permanently expanded in the papillary dermis, the uppermost layer of skin just beneath the surface. They appear as red or purple web-like patterns, typically less than one millimetre in calibre, and are flat against the skin.
They are the most common vascular presentation in aesthetic medicine.

What causes them: Chronic sun exposure, rosacea, hormonal changes, genetics, and the natural process of aging all contribute to telangiectasia formation. The vessel walls weaken, the capillaries dilate, and they become permanently visible beneath the skin.
What Vasculaze does: The 1064nm diode laser targets the oxyhemoglobin within the dilated vessel. The thermal energy coagulates the vessel wall, causing it to collapse. The body then reabsorbs the treated vessel over the following one to three weeks. Because the target is the hemoglobin — not the surrounding tissue — the skin above is largely unaffected.
What to expect: Telangiectasias respond excellently to Vasculaze. Most patients require one to three sessions. Mild redness for twenty-four to forty-eight hours is the typical recovery. There is no downtime.
Patient selection: Fitzpatrick skin types I through IV are appropriate candidates. In darker skin types, the risk of thermal injury to melanin-containing cells increases, and the benefit-to-risk ratio shifts unfavourably.
2. Cherry Angiomas
Cherry angiomas — also called senile hemangiomas — are benign proliferations of dilated capillaries in the papillary dermis. Unlike telangiectasias, they present as raised, dome-shaped lesions rather than flat patterns. They are characteristically bright cherry-red, firm to the touch, and range from one to five millimetres in diameter.
They are extremely common. If you are over thirty, you almost certainly have at least one.
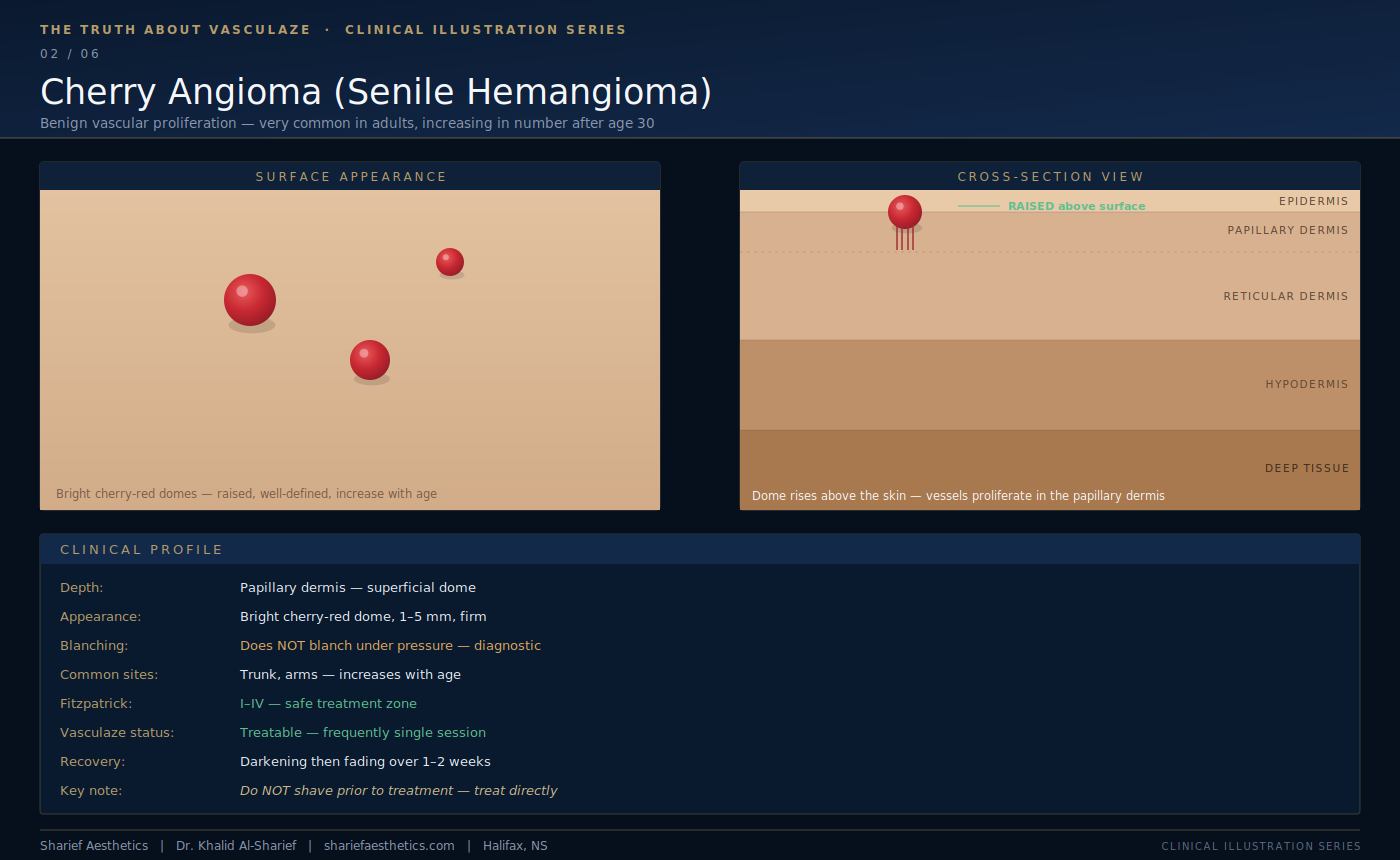
An important diagnostic note: Cherry angiomas do not blanch under pressure. This is a key clinical observation. A lesion that blanches when you press it — turning white momentarily before the red colour returns — contains blood that can be displaced. A cherry angioma does not blanch because the proliferating vessels are tightly packed and structurally abnormal. If a red lesion does not blanch, it warrants careful clinical assessment before any treatment.
What Vasculaze does: The laser energy targets the dense vascular proliferation within the dome. The lesion typically darkens immediately after treatment — this is normal and expected — before gradually fading and flattening over one to two weeks.
What to expect: Cherry angiomas often clear in a single session. They are among the most satisfying lesions to treat with this technology.
One important note for patients: Do not shave, scratch, or attempt to remove a cherry angioma at home before coming in. Treat it as you found it. We assess it clinically first.
3. Port Wine Stains
Port wine stains are capillary malformations — a structural error in the development of blood vessels that occurs before birth. They are present at birth, they never involute, and they are not hemangiomas. The distinction matters clinically because the biology is completely different.
A port wine stain is a flat, irregularly-shaped patch of pink, red, or purple discolouration. It does not rise above the surface of the skin. It does not grow the way an infantile hemangioma grows. But it does change over time — without treatment, port wine stains darken progressively and, in adulthood, can develop a thickened, nodular texture.

I have personal experience with this condition. I have a hereditary port wine stain on my neck. I have had it treated. I say this not to sell you on the procedure — I say it because I believe a physician who has experienced what they recommend brings a different level of informed consent to the conversation.
What Vasculaze does: The laser targets the dense network of capillaries throughout the dermis. Because port wine stains involve the full thickness of the dermis — not just the superficial papillary layer — multiple sessions are required. Complete clearance is rarely achieved, but significant lightening is consistently possible.
What to expect: Progressive lightening over a series of treatments. Earlier treatment produces better outcomes — younger tissue responds more readily, and the condition has not yet progressed to its thickened adult form.
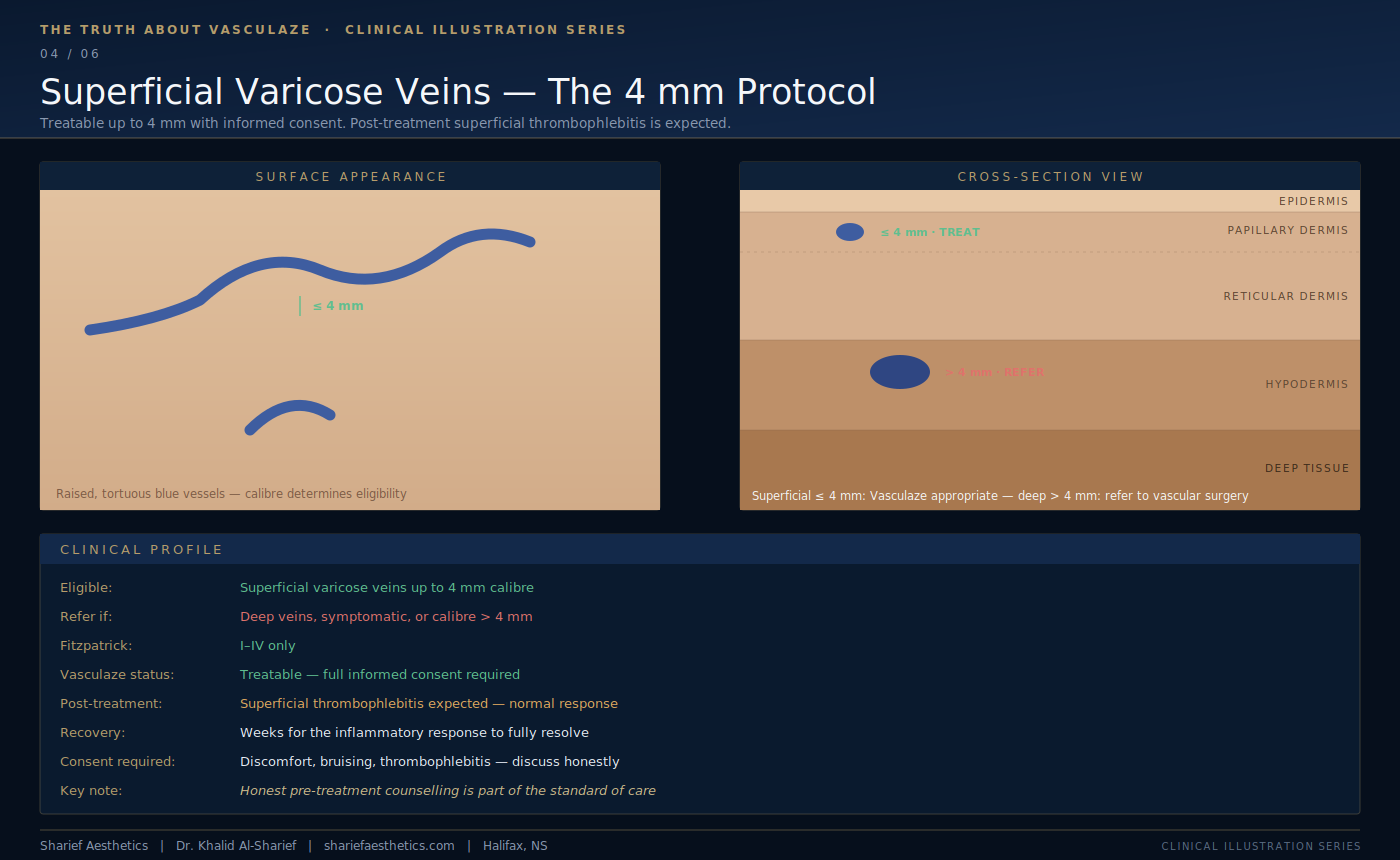
4. Superficial Varicose Veins — The 4mm Protocol
Varicose veins are dilated, tortuous veins — vessels that have lost their structural integrity and become permanently enlarged. They appear as blue or green rope-like structures visible beneath the skin, most commonly on the legs.
Here is where I want to be precise, because the clinical literature and device marketing are not always aligned on this point.
Vasculaze is not appropriate for deep or large varicose veins. Patients with symptomatic varicose veins — aching, heaviness, swelling, skin changes — should be assessed by a vascular surgeon. This is a medical condition, not an aesthetic one.
However, for superficial varicose veins up to four millimetres in calibre, Vasculaze can be an effective treatment option.
What patients need to understand: When a laser coagulates a superficial varicose vein, the treated vessel develops superficial thrombophlebitis — a localised inflammatory response within the vein as the body processes the treated tissue. This presents as tenderness, redness, and firmness along the treated vessel. It is an expected and normal part of the healing process, not a complication. It resolves over several weeks.
I discuss this explicitly with every patient before treating superficial varicose veins. Informed consent is not optional. A patient who is not prepared for a period of localised discomfort will interpret a normal healing response as something going wrong. That is a failure of communication, not a failure of treatment.
What to expect: Gradual fading of the treated vessel over weeks to months. The inflammatory response resolves fully. The underlying vessel is absorbed by the body.
5. Hemangiomas — Size and Depth Determine Everything
Hemangiomas are benign vascular tumours. Unlike malformations, they are not present at birth — they appear in the first weeks of life, proliferate rapidly, and then slowly involute. Most resolve on their own by early adolescence.
In an aesthetic practice, the hemangiomas I encounter are adult presentations — either residual involuted lesions from childhood, or the more common adult variants such as cherry angiomas (discussed above) and lobular capillary hemangiomas.
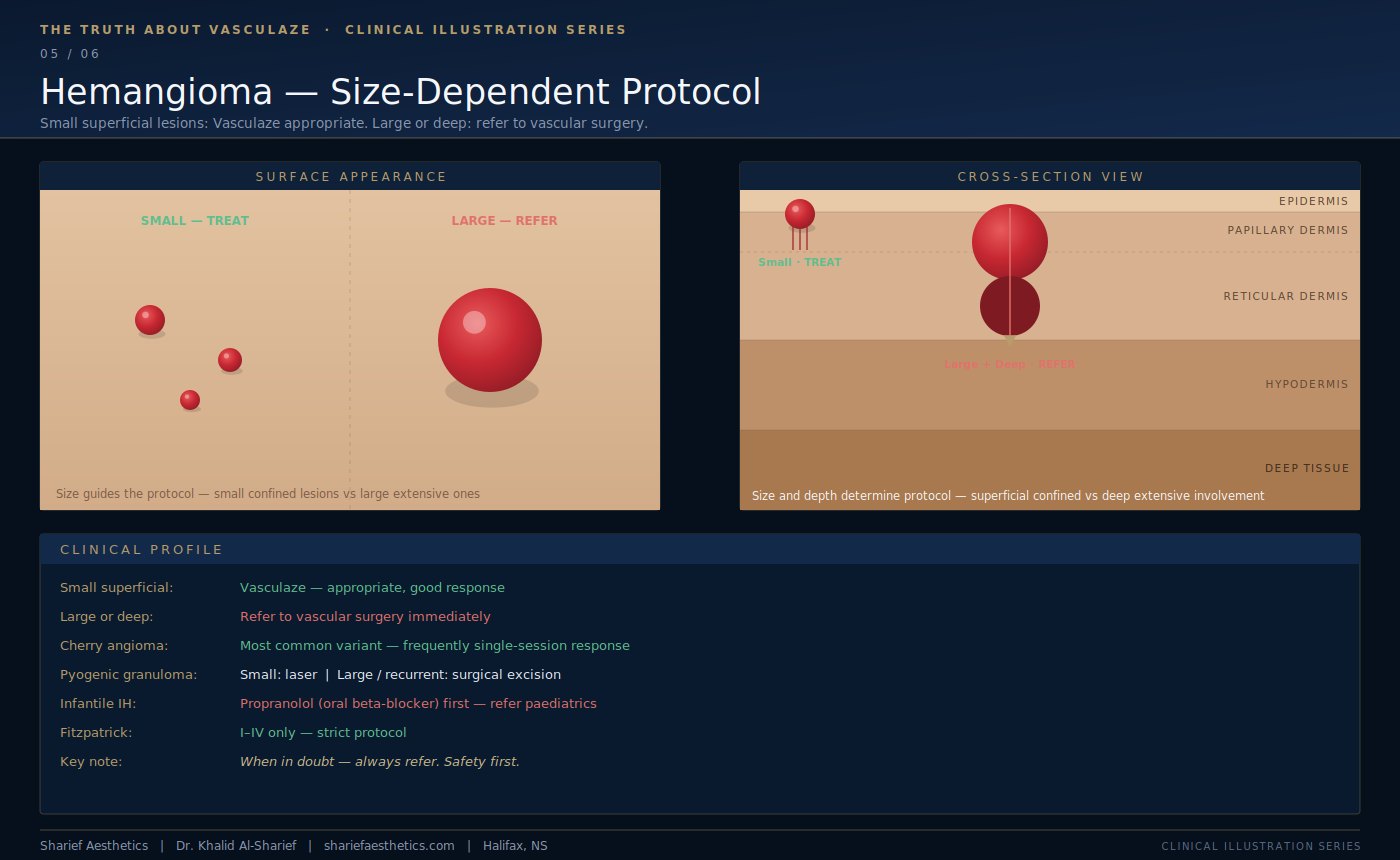
The size-dependent protocol:
For small, superficial hemangiomas — the kind that are confined to the papillary and upper reticular dermis — Vasculaze is an appropriate treatment with good results.
For large or deep hemangiomas — lesions that extend into the hypodermis or deeper, or that are significantly elevated and vascular — the appropriate course of action is referral to a vascular surgeon or a specialist in vascular anomalies. Attempting to treat a large deep hemangioma with surface laser is not only ineffective — it can cause surface injury without addressing the underlying lesion.
A note on infantile hemangiomas in children: The current standard of care for complicated infantile hemangiomas is oral propranolol — a beta-blocker that has revolutionised the management of this condition. If a parent brings a child with a growing hemangioma to an aesthetic clinic, the correct response is referral to paediatrics, not laser treatment. This is not an aesthetic presentation. This is a medical one.
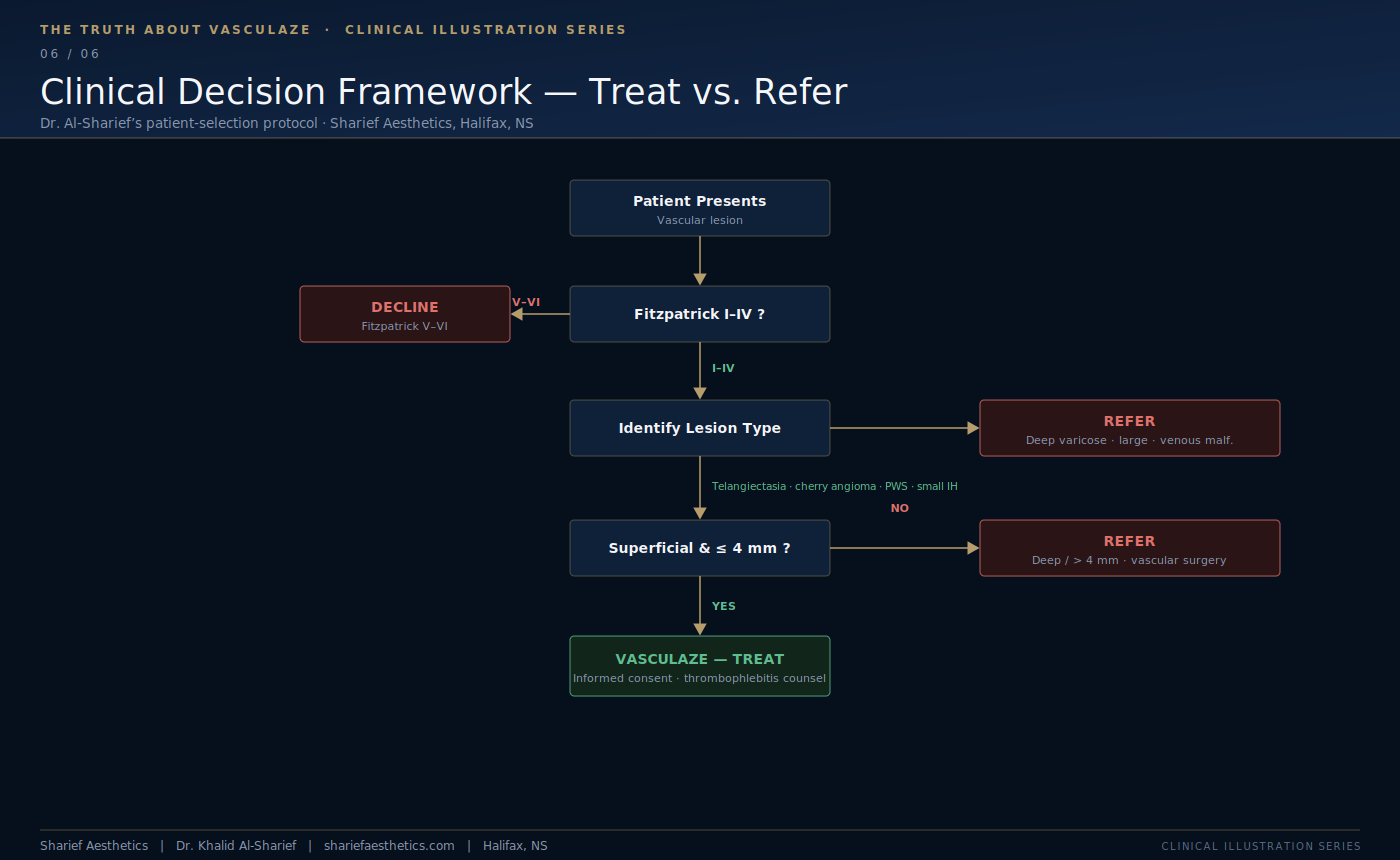
The guiding principle: When in doubt — refer. The patient's safety is not negotiable.
6. When Vasculaze Is Not the Answer
There are two additional categories worth addressing — not because they are commonly treated, but because patients sometimes present asking about them.
Venous malformations are blue-purple, soft, compressible lesions caused by abnormally formed veins. They are often mistaken for hemangiomas but are structurally different. They do not respond to surface laser treatment. The appropriate treatment is sclerotherapy — an injection-based technique that collapses the abnormal vessels from within — or surgery. These patients should be referred to a vascular specialist.
Deep varicose veins — veins larger than four millimetres, or veins associated with symptoms of venous insufficiency — are outside the scope of aesthetic laser treatment. These patients need proper venous assessment and may require endovenous ablation or surgical intervention.
What This Means for You as a Patient
If you are considering treatment for a vascular lesion, the most important thing you can bring to your consultation is a clear description of the lesion — how long you have had it, whether it has changed, whether it is flat or raised, and whether it causes any symptoms.
A physician-led consultation will assess your lesion clinically before recommending any treatment. We will classify what you have, explain the appropriate options, and be honest about what is achievable and what is not.
Some lesions clear in a single session. Some require a series. Some are not appropriate for laser treatment at all and belong in a different clinical setting entirely.
That honesty — delivered before treatment, not after — is what physician-led aesthetic medicine looks like in practice.
To learn more, contact the team at Sharief Aesthetics.